
Spinal Cord
last authored:
last reviewed:
Introduction
The spinal cord is continous with the medulla in the brain stem and runs from the base of the skull to the body of the first vertebra.
It contains 31 segments that each have a motor and sensory nerve root, which combine to form 31 pairs of spinal nerves.
Spinal Cord Anatomy
The spinal cord is approximately as round as your finger.
It begins at foramen magnum and extends to L1/L2, at which point the conus medullaris tapers into the filum terminalis, a connective tissue tether. begins and forms the cauda equina.
The spinal cord is covered with pia, arachnoid, and dura. The epidural space contains blood vessels and fatty tissues. Denticulate ligaments, continuous with pia, connect the spinal cord with the meninges.
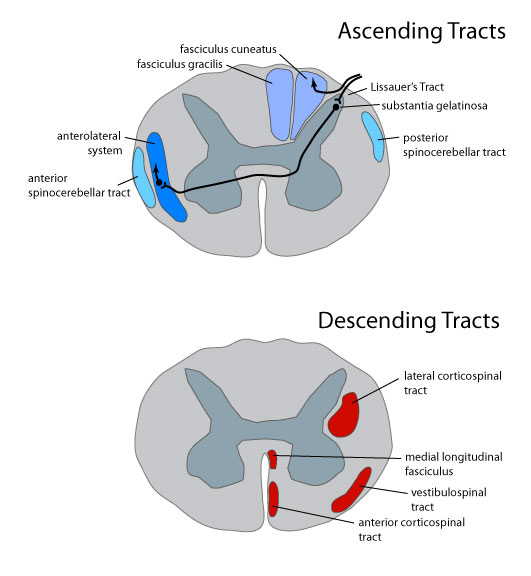
Spinal Cord Tracts
Descending signals are involved in motor control, while ascending signals provide sensory information. These are organized into major tracts.
main articles: motor control bodily senses
Descending, efferent fibres leave the spinal cord through ventral roots. They include:
- motor neurons, whose bodies are in the ventral gray horn. The most important of these is the corticospinal tract.
- preganglionic autonomic neurons, whose bodies are in lateral gray horns
- medial longitudinal fasciculus, involved in eye movements
Asecending systems convey sensory information. Afferent neurons, entering the dorsal root, have their cell bodies in dorsal root ganglia. Ascending fibres tend to synapse prior to decussating (crossing to the contralateral side). The major ascending pathways are as follows:
- spinothalamic tract - pain, temperature, crude touch
- dorsal column and medial lemniscal system - proprioreception, fine touch, vibration
- spinocerebellar tract - proprioreception
Medical sciences has traditionally viewed nerve pathways dedicated to specific sensory functions as being segragated in different areas of the spinal cord. In fact, most kinds of sensory information reach the thalamus and cerebellum by more than one route. As a result, loss of single tract can often be compensated for, often to a very large degree, by other areas.
Spinal Cord Nuclei
Spinal cord nuclei are found in the gray matter, and are sensory and motor, and autonomic.
Sensory Nuclei
The substantia gelantinosa receives information through Lissauer's tract. It contains relatively small neurons and stains more lightly becuase it deals with finely myelinated/unmyelinated fibres related to pain.
It is local processing nucleus; synapses with other nuclei for further transmission. It extends logitudinally throughout spinal cord, capping dorsal horn. It is continuous in medulla and pons with the spinal nucleus of the trigeminal.
Dorsal proper nucleus has bilateral communication with the substantia gelatinosa and is involved in transmitting info over longer distances toward the brain.
The thoracic nucleus plays a proprioceptive role, especially regarding the lower limb. It is found largely in thoracic segments of the spinal cord. T posterior cerebellar tract ascends ipsilaterally to cerebellum
The lateral horn is located in the intermediate gray of T1-L3. It contains sympathetic preganglionic neurons, as parasympathetic neurons in S2-S4.
Motor Nuclei
Motor nuclei are composed of lower alpha motor neurons with large cell bodies - 40-60 um across.
The medial motonuclear group is found at almost every level of the spinal cord, with distribution to the axial skeleton.
The lateral motonuclear group is found primarily cervically and lumbosacrally; due to their number they form enlargements within the spinal cord. They innervate the innervate limbs. Flexors tend to be dorsal, while extensors are ventral.
Conditions Affecting the Spinal Cord
The different points of decussation aids in determining whether a problem is in the brain stem or spinal cord. A brain stem lesion will lead to contralateral deficits in touch, pain, and proprioreception, while a spinal cord lesion will lead to contralateral loss of pain but ipsilateral loss of proprioreception and touch.
Spinal shock is the period of flaccid paralysis, lasting a few days following spinal cord transection. Deep tendon reflexes then return and become hyperreflexive. This is not well understood.
Brown-Sequard Syndrome is a rare but informative condition where half the spinal cord is transected. Tactile, vibratory, and proprioreceptive information is lost ipsilaterally from the dorsal column, while pain and temperature are lost contralaterally from the spinothalamic tract.
Syringomyelia is a disease of the central part of the spinal cord in which a tube progressively enlarges. Bilateral pain and temperature sensation is usually the first to go due to the crossed fibres, followed by weakness and muscle atrophy due to progressive anterior horn damage.
Resources and References
 |