
Breast Cancer
last authored:
last reviewed:
Introduction
Breast cancer is the most common cancer in women in the developed world.
Causes and Risk Factors
Risk factors for breast cancer include:
- female gender
- age
- prior history of breast cancer
- first degree relative wuth breast cancer
- nulliparity
- first pregnancy >age 30
- menarche < age 12
- menopause > age 55
- radiation exposure
- history of atypical hyperplasia/papilloma
- >5y hormone replacement therapy
- obesity in post-menopausal women
BRCA is an autosomal dominant gene with a lifetime risk of 85% developing breast cancer.
- 5-10% of breast cancers appear caused by inherited genetic mutations, in genes including BRCA1, BRCA2, p53, PTEN, and CHK2
- penetrance is affected by modifier genes, carcinogens, response to DNA damage, and hormonal/reproductive factors
Male breast cancer risk factors include:
- hormone exposure (overwright, exogenous hormones, liver disease, alcohol intake)
- Klinfelter's syndrome
- radiation exposure
- family history
Pathophysiology
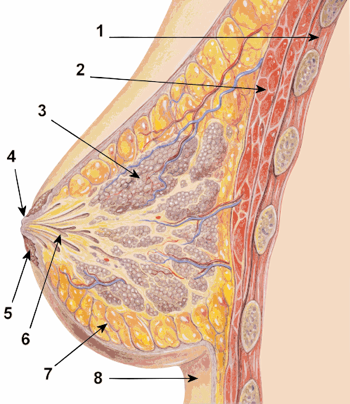
image by Patrick Lynch, downloaded from wikipedia
{kind=link}
Ductal hyperplasia can be present.
Screening
While screening and early diagnosis is robust in many countries, in others, presentation is often too late. Indian oncologist Ravi Kannan states, for example “Women sometimes come in with lumps in their breast that are 30—35 cm large. These heavy masses of cancerous cells protrude outside the body, ulcerating or teeming with maggots” (Shetty, 2012).
Breast cancer screening is quite controversial in regards to recommendations.
There is no clear screening guidelines as pertaining to clinical breast exam.
Regarding mammography, according to the Alberta clinical practice guidelines:
- under 40: should not receive mammography
- 40-49: discussion regarding risks and benefits of mammography
- 50-69: screening mammogram at least every two years
- over 69: screening mammogram should be considered every two years, depending on patient and her preferences
- if there is a strong family history, screening should commence 5-10 years prior to the earliest breast cancer
MRI can also be used, though predominantly in high-risk patients. MRI and mammography can be staggered.
For BRCA mutations, mammography is less than 50% sensitive, while MRI catches approx 90%.
Signs and Symptoms
- history
- physical exam
History
A breast lump is typically the initial presentation of breast cancer. It can be identified by screening during a clinical exam or mammogram, or by the patient her/himself.
Questions to ask include:
- how has it been growing or changing?
- nipple discharge
- when and how was it noticed?
- last clinical breast exam, last mammogram
Review of systems may reveal:
- weight loss
- lack of appetite
- bone pain
Other questions should include:
- past breast history
- past obstetrical history
- age of menarche
- medications, especially birth control pill, hormone replacement therapy
Physical Exam
breast exam
- soft vs firm
- mobile vs non
- skin changes
lymph nodes: axillary and supraclavicular
respiratory exam: pleural effusion
Investigations
- lab investigations
- diagnostic imaging
Lab Investigations
Fine needle aspiration (FNA) is simple procedure with low risk of complications. However, it has a false negative rate of ~10% and doesn't disinguish between in situ and invasive disease.
Biopsy is a more diagnostic procedure, and includes core, excisional, and incisional approaches.
A finding of atypical ductal hyperplasia requires further excision, as malignancy could simply be adjacent to the area originally sampled.
Pathological indices of importance include:
- margins
- grade
- lymphovascular morphology
- estrogen receptor + or -
- Her2/neu + or -
Diagnostic Imaging
Mammogram should be performed before biopsy of any type.
Up to 15% of breast cancers are mammographically occult.
CXR for lung mets.
Staging should include bone scan, chest X-ray, and CT of the abdomen and pelvis.
Staging
Staging depends initially upon history and physical exam.
Types of Breast Cancer
Ductal carcinoma in situ (DCIS)
DCIS involves malignant cells that are completely contained with breast ducts. It is generally diagnosed by screening mammography, as DCIS is usually asymptomatic.
Cells are often high grade and multifocal.
Lobar carcinoma in situ (LCIS)
LCIS is almost always an incidental finding on biopsy, as it is asymptomatic and not seen on mammogram. It commonly is diagnosed before menopause, ages 40-50. It is a field effect, predisposing for invasive malignancy in both breasts, in all four quadrants.
Invasive ductal carcinoma (IDC)
IDC is the most common type of breast cancer, representing invasion into surrounding tissues. It is more common above age 55 and is often diagnosed on screening mammogram, followed by biopsy.
Symptoms, if present, can include swelling, dimpling, pain, and nipple inversion.
Invasive lobular carcinoma (ILC)
ILC begins in the breast lobules before spreading. It is the second-most common breast cancer type. It tends to have a later age of onset (mid-60s).
ILC is more challenging to detect on mammogram, as they do not form a lump. Symptoms include a sense of fullness or swelling. Dimpling or nipple inversion may also be present.
Inflammatory breast cancer
This is the most aggressive, and thankfully rarest, type of cancer. It usually begins with a thickness or heaviness in the breast, rather than a lump. Other symptoms include swelling, erythema, aching, burning, and nipple inversion, and 'peau d'orange' skin.
Paget's disease of the breast
Paget's disease is a desquamating, erythematous condition of the nipple, predominantly in older women. Biopsy demonstrates non-malignant pagetoid disease. It always suggests underlying ductal disease.
Treatments
Treatment depends on stage of diease and risk factors.
DCIS
Early stage cancer without lymph node spread is equally treated with:
- lumpectomy plus radiation vs
- mastectomy
Chemotherapy is generally not required.
LCIS
LCIS can be treated with increased surveillance, tamoxifen, or with bilateral mastectomy.
Lumpectomy is contraindicated in patients with:
- condition preventing radiotherapy (pregnancy, previous radiotherapy, inability to lie flat)
- tumour to mastectomy ratio
- multifocal disease
Invasive ductal carcinoma and invasive lobar carcinoma
IDC and ILC may be treated with
- lumpectomy + radiation
- mastectomy +/- radiation
- sentinel node biopsy
- tamoxifen if ER +
- Herceptin if Her2/neu +
- chemotherapy if
- ER positive and young
- ER negative and node positive
- high risk node positive
- high grade lesion
- lymphovascular invasion
- palliation
Surgery is performed to remove the tumour and to evaluate/remove lymph nodes. Surgery shouldn't be used if patients are medically unfit, in advanced or locally invasive cancers, or inflammatory conditions.
Inflammatory breast cancer
Inflammatory malignancy should NOT be treated with any type of surgery, as it is non-curative and result in tumour growth in the would and disastrous healing. Chemotherapy is the first line. Hormone treatment and radiation are also often used.
BRCA1
Women should be advised to have bilateral mastectomy and oophorectomy.
There is no contraindication to pregnancy in these women.
Consequences and Course
The following relates to course with recommended treatments:
- DCIS: 90% 5-year survival
- LCIS:
- IDC: dependent on size, nodes, and metastasis
Resources and References
Shetty P. 2012. India faces growing breast cancer epidemic. Lancet. 379(9820):992 - 993.
Topic Development
authors:
reviewers:
 |