
Cord Prolapse
last authored: July 2010, Kim Colangelo
last reviewed: Nov 2011, Shannon MacFarlane
Introduction
Cord prolapse is a rare obstetrical emergency. It occurs when a part of the umbilical cord falls adjacent to or below the presenting part of the baby. This results in compression of the cord between the presenting part and the pelvis leading to hypoxia in the baby.
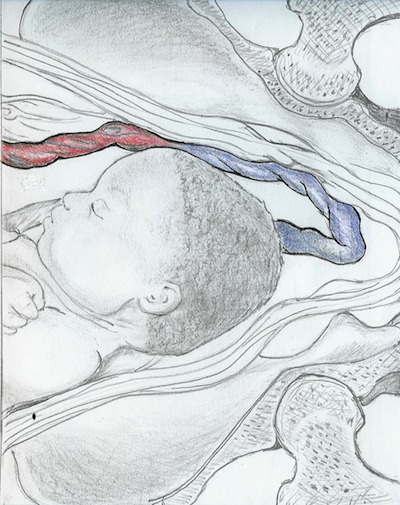
overt prolapse, by Mary Chia
An overt prolapse is when the cord is below the presenting fetal part, usually through the cervical os into or through the vagina. Loops of cord are palpable on pelvic exam or are visually protruding through the introitus. Rupture of membranes is a prerequisite for overt prolapse.
An occult prolapse is when the cord lies alongside the presenting fetal part. The membranes may be intact or ruptured. This type of prolapse is often more difficult to detect, and is rarely palpated. Occult prolapse is usually detected by fetal heart changes associated with cord compression.
The Case of Mrs White
A 34yo multip presents to labour and delivery after spontaneous rupture of the membranes. She is having irregular contractions for the last hour. Her complete history was taken at triage. The triage nurse performs a vaginal exam to assess her labour status. The cervix is 5cm, and when determining the presenting part she feels a slippery, pulsatile mass.
- What is the main concern in this situation?
- What should the next step be?
Causes and Risk Factors
Breech presentation confers a higher risk of a cord prolapse, with a footling breech being the highest risk compared to a frank or a complete.
- prematurity
- multiple gestation (with the second born twin having a higher risk)
- malpresentation
- cephalopelvic disproportion
- polyhydramnios
- premature rupture of the membranes (PROM)
- multiparity
- placenta previa or low lying placenta
- pelvic mass or pelvic deformity
- obstetric procedures: articifical rupture of membranes, version, rotation, forceps, intrauterine pressure monitoring, scalp electrodes
- long cord
Pathophysiology
There are numerous risk factors for a cord prolapse leading to several pathophysiologies.
It is important to understand the structure and function of the umbilical cord to understand why a cord prolapse is an emergency. The umbilical cord consists of an umbilical vein which carries oxygenated blood, and 2 umbilical arteries that return deoxygenated blood (in a normal 3 vessel cord). The umbilical vein is thin walled and especially susceptible to compression. At higher pressures the arteries will also be compressed. The decreased in blood flow triggers baroreceptors causing vagal stimulation which causes decelerations (lower heart rate). Chemoreceptors can sense hypoxemia and thus may raise the baseline heart rate to a tachycardic range.
If the presenting part does not fill the entire cervix there is room for the cord to descend, hence the highest risk is in a footling breech (where the foot is the presenting part). Prematurity and multiple gestation confer a higher risk of breech and therefore higher risk of cord prolapse.
Additional factors that cause the presenting part to not be fully engaged when the rupture of membranes occur and the cord is at risk for descent are PROM (which is more likely in multiparous), obstetrical interventions that can disengage the presenting part, placenta previa or low lying placenta, and a large pelvic mass or deformity. A complete previa would prevent overt prolapse; however, occult prolapse can still occur.
Polyhydramnios as a risk factor is thought to be related to the large volume of amniotic fluid that flows out when the membranes rupture, the force then pushes the cord down. Prematurity as a risk factor could also be related to a relative polyhydramnios compared to the size of the fetus.
Signs and Symptoms
- history
- physical exam
History
It would be rare for a patient to say that they feel a cord prolapse; it is more commonly diagnosed when an abnormal fetal heart tracing is seen leading a health care professional to perform a vaginal exam and then feel the cord.
Physical Exam
Mother:
A visible or palpable cord at or below the level of the presenting part of the fetus on vaginal exam. The cord feels slippery and pulsatile. It is more difficult to feel an occult cord prolapse.
Fetal Heart Monitoring
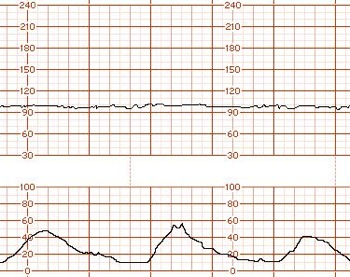
The top tracing is the fetal heart, the bottom is
uterine activity (peaks = contractions. A normal fetal heart
rate has a
baseline of 110-160; the baseline on this is 100.
used with permission, FMDRL
The fetal heart rate changes due to hypoxia from cord compression. This can include bradycardia, as seen on the left, or variable decelerations.
A variable deceleration is a decrease in the heart rate greater than 15bpm, an onset to nadir of <30sec, and duration > 15sec but <2min.
Occult cord prolapse should be suspected in all patients with persistent or significant decelerations on external fetal monitoring.
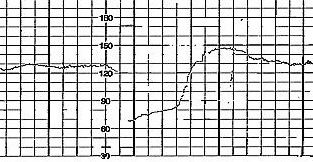
Fetal heart tracing showing variable deceleration
with an overshoot.
used with permission, FMDRL
A non-reassuring variable deceleration, as on the right, can have:
- a prolonged return to baseline, >60sec
- a rising baseline rate to the tachycardic range, >160bpm
- an absent baseline variability
- an overshoot (returns to a rate higher than baseline)
Investigations
- lab investigations
- diagnostic imaging
Lab Investigations
Cord gases following the birth provide an idea of the degree of hypoxia the infant endured.
Diagnostic Imaging
A colour doppler can show the position of the cord. This is not recommended to investigate a suspected cord prolapse as it would result in a delay in definitive treatment, however a cord prolapse may appear when an ultrasound is ordered for another reason.
A routine ultrasound prior to the onset of labour may show a cord as a presenting part. A follow up scan is booked to reasses the cord presentation and a caesarean delivery may be planned if the presenting cord persists. There is currently no guideline recommending screening for cord prolapse.
Differential Diagnosis
The differential diagnosis for fetal bradycardia includes:
- maternal hypotension (possibly following an epidural)
- placental abruption
- uterine rupture
- vasa previa
Treatments
This is an obstetrical emergency! There are several techniques to promote adequate oxygenation to the fetus during this time. The combination and order that is appropriate for each situation will vary depending on the resources and the estimated time a safe delivery can be prepared.
Perform pelvic exam to determine:
- cervical effeacement and dilation
- station of presenting part
- presence of pulsations within cord vessels
Monitor the fetal heart.
If there is fetal demise allow labour and delivery. If the fetus is too premature for viability
(generally at <22 weeks), expectant management versus termination of the pregnancy should be discussed with the mother.
If fetal
viability is possible arrange an emergency caesarean section. If vaginal delivery is imminent and immediately feasible, then it is acceptable to proceed with vaginal delivery while Caesarean section is being organized. If Caesarean section is not possible, attempt delivery as best as is possible. Call for assistance, as help will likely be needed for neonatal resuscitation.
Relieve the cord compression. If the cord is outside the introitus, gently place it back inside the vagina as cold and handling can cause cord vasospasm. Warm saline soaks can also be applied inside the vagina. Put your hand inside the vagina and elevate the presenting part off of the cord until delivery. Do not manipulate the cord.
Give oxygen to the mother and consider administering tocolytics to reduce contractions while preparing for the caesarean section. Position the mother in the Trendelenburg (flat on back with the feet higher than the head) or knee-to-chest position. This moves the fetus back to try and relieve some of the cord compression.
If there will be prolonged time for Caeasarean section, or transport is required, the
bladder can be filled with 500-700 cc of normal saline via a Foley catheter - similar
to the effect of positioning this will help elevate the fetus off of
the cord.
If
a caesarean delivery is not possible, a funic reduction can be
performed. This involves putting the cord along the nuchal area of the
fetus and keeping the fetal head elevated.
Prevention can
occur in certain identified high risk situations by
puncturing the membranes with a needle to prevent the forceful gush of
amniotic fluid that is associated with cord prolapse. Breech
presentations should have a vaginal exam after rupture of the membranes
to rule out a cord prolapse and continuous electronic fetal monitoring
so abnormal tracings that could be indicative of a prolapse are
identified early.
Consequences and Course
The main concern with a cord prolapse is cord compression leading to decreased blood flow to the fetus and cord vasospasm, both of these leading to hypoxia in the fetus. The elapsed time between a cord prolapse and relief of the compression is an important determinant for the outcome, however the degree of cord compression also plays a role. The risk factors for a cord prolapse often carry an inherent risk as well, for example a premature infant has other risk factors for injury.
Although fetal hypoxia can affect any organ system, the main concern is for hypoxic-ischemic encephalopathy (HIE). Much of the damage to the myocardium, renal, pulmonary and GI systems is transient whereas HIE often leads to permanent neurological sequelae such as cerebral palsy.
Resources and References
- Royal College of Obstetricians and Gynaecologists. Green-top guideline number 50. April 2008.
- Family Medicine Digital Resource Library. FHR monitoring article, Dr. Brian Crownover.
- MoreOB
Topic Development
authors: July 2010, Kim Colangelo
reviewers: Nov 2011, Shannon MacFarlane
 |