
Head & Neck Squamous Cell Carcinoma
last authored, August 2009, David LaPierre
last reviewed:
Introduction
Almost all head and neck cancer is squamous cell carcinoma (SCC) originating from basement membrane cuboidal cells. The most common sites include the oral cavity and larynx.
Rates are increasing as the population ages.
Causes and Risk Factors
Head and neck cancers are most common in middle-aged and elderly people who have excessively used cigarettes and alcohol, though these are by no means the only causes.
Other risk factors include:
- poor dental hygiene
- chewing betel nuts
- infections: HIV, herpes simplex, Epstein-Barr virus
- immunosuppression
- chronic inflammation (e.g. lichen planus)
- oral submucous fibrosis
- discoid lupus erythmatosus
- tertiary syphilis
Head and neck cancers are within the top five malignancies in developing countries, and rates are also increased in areas of low socio-economic status.
Pathophysiology
Pre-malignant conditions include leukoplakia and erythroplakia - white and red patches, respectively.
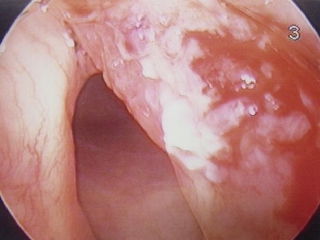
Laryngeal squamous cell carcinoma
image used with permission
Dr. Ghorayeb, Otolaryngology Houston
Possible sites of origin include:
Oral Cavity: lips, tongue, floor-of-mouth, maxillary alveolar ridge/hard palate, mandibular alveolar ridge, buccal vestibules.
Pharynx: Nasopharynx (Eustachian tubes and adenoid, skull base).
Oropharynx: tongue base, soft palate, palatine tonsils, posterior wall of pharynx
Hypopharynx: piriform sinuses + postcricoid area leading into esophagus below
Larynx: supraglottis (epiglottis, false vocal cords): cancers here spread early to LNs.
Glottis (true vocal cords): commonest site of laryngeal cancer. Present with hoarseness.
Subglottis: up to 1 cm below vocal cords, leads into trachea below: cancers here are rare
Signs and Symptoms
- history
- physical exam
History
Symptoms are cuased by irritation, swelling, and ulceration, and depend on site of origin. These include:
Larynx: hoarseness, sore throat, dyspnea (late presentation)
- swelling
- unilateral ear pain/hearing loss from blocked eustachian tube
- dysphagia
- odynophagia
- persistent oral ulcer
- unilateral serous otitis
Physical Exam
neck mass
Investigations
If lesion small or in inconsequential area: excisional biopsy
If lesion large or in esthetically sensitive area (eyelid): punch biopsy
Biopsy confirms diagnosis but more importantly assesses depth (1° determinant of prognosis)
- lab investigations
- diagnostic imaging
Lab Investigations
Diagnostic Imaging
Differential Diagnosis
The differential for a neck mass includes:
- inflammatory neck nodes
- lymphoma
- salivary gland disease: infection, tumour
- thyroiditis, goitre, cancer
- metastasis
Stage and Grade
Head and neck SCC is staged using the TNM system:
- T1-4: tumour size
- N0-3: lymph node involvement and size
- M0-1: metastasis
Treatments
HNSCC are treated by various treatments.
Oral cavity tumours are treated by surgery, with radiotherapy added if pathology suggests spread. Surgeries often involve skin flap transfer, often from the radial forearm.
Laryngeal cancers are often treated by endoscopic laser, with total laryngectomy performed with advanced disease.
radiation or surgery for early stage and chemotherapy or surgery plus radiation for late stage.
All patients with tumours obstructing their airways should undergo a tracheostomy while awake, followed by general anesthesia and endoscopy for tumour stage and grade.
Consequences and Course
Prognosis, like all cancers, depends on stage of disease. Cervical node metastasis decreases survival by 50%.
Untreated squamous cell carcinoma tends to metastasize to the liver, lungs, bone, and brain.
Secondary cancers are also common, occurring at a rate of ~4%/year.
As many people who develop head and neck cancers are older and have other co-morbidities, the focus of disease treatment is often non-curative.
Resources and References
NICE Improving Outcomes in Head and Neck Cancers
Topic Development
created: Aug 2009, David LaPierre
authors:
editors:
reviewers:
 |