
Acute Otitis Media
last authored: Oct 2009, David LaPierre
last reviewed:
Introduction
Acute Otitis media (AOM) is an infection of the middle ear, normally following blockage of the eustacian tube by infection, pharyngitis, or adenoid hypertrophy. It is usually caused by bacteria, though viruses may also be responsible for sym.ptoms.
Otitis media is primarily a disease of children, with incidence peaking between 6-12 months. Over half of children have had an ear infection by age one.



A certain diagnosis is made with three criteria:
- recent, sudden onset signs and symptoms
- presence of middle ear effusion
- middle ear inflammation
Recurrent AOM occurs in over 10% of the population, and is defined by 3 episodes in 6 months, 4 episodes in 1 year, or 6 or more episodes in the first 6 years of life. Otitis media with fluid collection over 3 months is considered otitis media with effusion.
The Case of Nathan Benstead
Nathan is 15 month-old who had been sick with a runny nose and cough for a week. He appeared to be getting better, but then developed a fever and terrible right ear pain. His mother brought him to the family doctor, concerned about an ear infection.
What should the doctor do?
Causes and Risk Factors
Bacteria are responsible for up to 70% of infections. The most common pathogens include:
- S. peumoniae
- non-typable H. influenzae
- M. catarrhalis
Other less frequent causes include Streptococcus pyogenes.
Viral causes include rhinovirus and RSV, and can occur alone or alongside bacteria.
Major risk factors for developing AOM include:
- bottle-feeding
- cigarette smoke at home
- sick contacts (ie daycare)
- family history
- sibling at home, especially sharing a room
- cleft lip
AOM is more common in males. Other higher risk populations include:
- lower SES
- immunosuppresed children
- Down's syndrome
- Native Americans
- prematurity
Pathophysiology
Once blocked, air in the middle ear is absorbed. This creates negative pressure and also draws bacteria up from the nasopharynx into the middle ear. Stasis leads to localized bacterial proliferation, inflammation, pus collection, and symptoms.
Signs and Symptoms
- history
- physical exam
History
Symptoms are quite non-specific in infants, consisting of fever, fussiness, decreased feeding, and ear tugging. Vomiting, nausea, and diarrhea may also occur.
Older children and adults can complain of ear pain and decreased hearing.
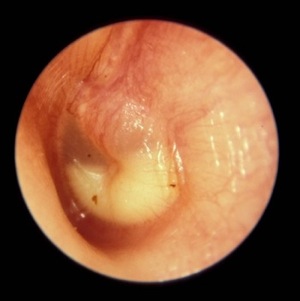
Physical Exam
A fever is a telling sign of AOM, but not as much as tympanometry.
Middle ear effusion:
|
Middle ear inflammation:
|
Investigations
- lab investigations
- diagnostic imaging
Lab Investigations
none usually required
Diagnostic Imaging
none usually required
Differential Diagnosis
- temperomandibular joint dysfunction
- pharyngeal/laryngeal carcinoma
Treatments
Pain control is a key treatment, with acetominophen and ibuprofen.
There is often uncertainty regarding antibiotic treatment of AOM, as 60-80% of children resolve with suppoertive therapy.
Amoxicillin is the first-line antibiotic, used to cover S. pneumoniae. Ceftriaxone can be used as second-line, or in patients with penicillin allergy.
If patient is under 6 months of age, or if follow-up is uncertain, antibiotics should be provided.
Ciprodex ear drops are ideal for suppurative otitis media.
Gentamycin should be AVOIDED, as it is ototoxic.
Consequences and Course
90% of suppurative otitis media heals within months. The remainder results in chronic suppurative otitis media (active, quiescent, inactive)
Chronic inflammation can result in tympanosclerosis (myringsclerosis), or calcified ear drum. THis can result in conductive hearing loss.
Resources and References
Topic Development
created:
authors:
editors:
reviewers:
 |