
Nutrition in Health Care Education
Nutrition plays a key role in many chronic conditions and diseases, including obesity, type II diabetes, hypertension, osteoporosis, and many others. While pharmacological advances continue for many of these conditions, cumulative evidence shows that much of the morbidity and mortality of these conditions is preventable through diet and lifestyle choices. Large, well-designed landmark studies such as the Lyon Diet Heart Study (de Lorgeril et al, 1999), Lifestyle Heart Trial (Ornish et al, 1998), DASH (Appel et al, 2006), and Diabetes Prevention Program (Knowler et al, 2002) have shown the effects of diet on these disease to be beyond question. Although at present insufficient evidence exists to recommend dietary counseling for adults with no known risk factors, counseling interventions are effective in reducing disease risk and burden in adults with hyperlipidemia, hypertension, and other risk factors for nutrition-related chronic diseases (USPSTF, 2001). The public sees primary care providers as valuable sources of lifestyle advice, including nutritional guidance (Jackson, 2001; van Binsbergen et al, 2003; van Weel, 2003). However, significant barriers prevent many clinicians from offering dietary support. These include lack of time, lack of teaching materials, and lack of nutrition knowledge and confidence on the part of the provider (Kushner, 1995, Ockene et al, 1996). With rates of obesity and other risk factors soaring, most worryingly among children, a significant challenge facing health educators today is how to meet these barriers and equip health care providers to support healthy choices, addressing risk factors while primary prevention is still possible.
Nutrition in Health Education
While the need for health care providers to be equipped to offer nutritional support to patients is clear, the means of doing so is not. Educational programs for existing health care providers have thus far been equivocal (Harvey et al, 2001). Thus, pre-liscencure training in nutrition has been identified as essential by numerous organizations, including the American Society for Clinical Nutrition, the American Medical Student Association, the National Academy of Sciences, the American Academy of Family Physicians, the Society of Teachers of Family Medicine, and the US Congress (Krebs and Primak, 2006). A landmark report by the National Academy of Sciences recommended a minimum of 25 hours of nutrition training during medical school (National Academy of Sciences, 1985), while the American Society of Clinical Nutrition recommended at least 35 hours be provided (Weinsier et al, 1989). Indeed, the 2007 Medical School Objectives Project of the Association of American Medical Colleges (AAMC) focuses on learning objectives on obesity, including lifestyle changes (AAMC web site), and it is likely all medical schools will soon be required to train doctors about to offer effective nutritional counseling. The emphasis on outcomes-based educational objectives by the Liaison Committee on Medical Education (LCME) continues to encourage integration of knowledge into interprofessional, problem-based learning, and accreditation can be a positive experience as administrators, faculty, and students work together to create new directions for curriculum which meet these needs.
Integrating Nutrition into Curriculum
Even though nutrition is universally viewed as important in health care curricula, a large proportion of graduating medical students view their training in nutrition as inadequate (Adams et al, 2006). While a study is ongoing across Canadian medical schools to assess the nutrition education here, involving IWK physician Dr. Mohsin Rashid, among American schools, only 41% provide the minimum recommended 25 hours (Adams et al, 2006).
Medical school curricula are complex and full, and pressure to do more with less time makes addition of new information difficult. As well, there is a significant move away from lecture-based instruction to more problem-based learning. Implementation of dedicated nutrition courses is therefore unlikely, and nutrition content is thus best incorporated into preclinical and clinical training through integration into existing courses (Touger-Decker R, 2004; Krebs and Primak, 2006).
Lessons in successful approaches to this process have been well documented. Supported by the Nutrition Academic Award (NAA) supported by the National Heart, Lung, and Blood Institute, a number of medical schools underwent significant curriculum change, and their experiences made available for other schools to learn from (van Horn, 2006). Successful strategies which engage students include case-based learning, panels with patients, interprofessional symposia, and the use of standardized patients (Hark, 2006).
Learning Behaviour Modification Techniques
In order for nutrition advice to be useful, it needs to be followed consistently. As discussed, patients look to health care providers, notably family doctors, to offer this advice. It thus is critical for health care students to learn effective techniques to begin and maintain healthy behaviours, especially as nutrition counseling in primary care settings do improve risk factors (Eaton, Goodwin, and Stange, 2002).
These skills extend across various lifestyle choices affecting chronic illness, including smoking, alcohol and drug use, and stress. Minimal intervention counseling is a validated approach which incorporates motivational interviewing, the stages of change, and the five A's to provide focused behavioural change in little time (Whitlock et al, 2002). As health care providers confidently and effectively encourage change, discussions about diet and other lifestyle factors show results. Students therefore benefit from learning these skills early during their training and practicing them whenever possible.
Leading By Example
Students need to observe preceptors and mentors expertly offering nutritional advice in order to become well-skilled themselves, and many studies have demonstrated the need for champions such as endocrinologists, family physicians, geriatricians, nutritionists, epidemiologists, and others, to lead by example when it comes to nutrition (Krebs and Primak, 2006, Hark, 2006). Those passionate about nutrition need to be identified and encouraged to provide training to other preceptors in this areas. Champions for nutrition are also critical within the administration to facilitate a learning culture which embraces nutrition as fundamental to health (Hark, 2006).
Web-based Nutrition Education Resources
Web-based resources benefit from cost, accessibility, and ability to link to other resources and provide updates. According to the Canadian Medical Association Journal, 2/3 of Canadian physicians use the internet as a tool to support patient care (Martin S, 2004). However, almost as many agree that "searching the internet takes too much effort." (Chew et al, 2004). Accurate, easy-to-navigate and use materials, on a variety of nutrition topics, are required, and many American schools have created such resources, including the University of Wisconsin's Medical Nutrition Handbook and the University of North Carolina at Chapel Hill's Nutrition in Medicine (NIM). Lessons are case-based, incorporating brief nutrition counseling tools, potential investigations, and student evaluation tools.
In consideration of these lessons, web-based nutrition information is being developed for use by Dalhousie medical students and integrated with existing curriculum. The learning object 'fat' is a good example outlining this approach.
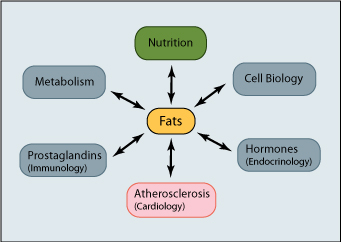 While understanding dietary needs and sources of fats, including unsaturated, saturated and trans fats, is critical, this must be viewed in the context of their roles in health and disease. Fats compose cell membranes, are precursors for steroid hormones and inflammatory molecules such as prostaglandins, and are central to disease processes such as atherosclerosis.
While understanding dietary needs and sources of fats, including unsaturated, saturated and trans fats, is critical, this must be viewed in the context of their roles in health and disease. Fats compose cell membranes, are precursors for steroid hormones and inflammatory molecules such as prostaglandins, and are central to disease processes such as atherosclerosis.
Fats in the diet are thus thought of together with disciplines such as immunology, cardiology, and endocrinology, providing important integration of nutrition with clinical health care and underlining its relevance.
Overview of Nutrition Education at Dalhousie Medical School
An introduction to nutrition occurs during Metabolism and Function, and while we discuss the role of macro- and micro-nutrients in energy production, storage, and use, there is some measure of disconnect from dietary sources and clinical application of this information. This is gap is addressed during Skin, Glands, and Blood through endocrine lectures on fats and nutrition. Nutrition is again discussed during the Cardiovascular-Respiratory block, which includes an excellent interprofessional workshop on behaviour modification. Many COPS cases excellently integrate nutrition, especially for cardiovascular, renal, and endocrine diseases. These lectures and cases are valuable as a basis for introducing the importance of nutrition to medical students. However, without the skills to discuss lifestyle and motivate patients to make and maintain healthy choices, this knowledge tends to remain underused.
Directions for the Future
1) Medical students respond well to a curriculum evaluating their own nutritional habits. One successful approach has been to ask them track food intake and activity for 24 hours before analyzing it for nutrient and energy intake (Conroy et al, 2004). This would fit well during the Metabolism and Function block and its focus on nutrients, potentially in COPS or minicase format. Food records can easily be printed to record information, and web-based analysis software is freely available through the Dietitians of Canada EATracker. Personalizing nutritional information encourages students to consider the role of dietary choices in caloric and nutrient intake, equipping them to help patients do the same.
{kind=link}
2) As has been discussed, giving effective lifestyle advice and encouraging behavioural changes are critical competencies for medical students. Case Practice uses simulated patients with which students experiment with new approaches and hone developing skills. Given the importance placed on diet during the SGB and CVR blocks, one of the Case Practice scenarios encountered by Med II students during these units could be as follows:
Mr/Ms Jean Levi is 45 y.o. and comes to your office to discuss some recent blood work. Reviewing the chart you notice that in the past four visits blood pressure readings have been at least 146/92. Total cholesterol, LDL and TG are higher than the acceptable ranges and s/he appears quite overweight. Your tasks are to:
- take a dietary history
- collect data and calculate Body Mass Index (BMI) and Waist Circumference (WC)
- based on these findings, provide minimal intervention counseling to Mr/Ms Levi
3) Lack of time is one of the important reasons cited by physicians as a barrier to offering nutritional support, and interprofessional care of patients in this area is of fundamental importance. Working together, we must ensure similar messages are being portrayed and reinforced as patients encounter different members of the health care team. The groundwork for interprofessional practice begins during education, and there is much promise in considering how students across the health faculties at Dal might learn about how to deliver nutrition support together. The emerging web site for the Dalhousie Health Sciences Students Association, www.HealthAtDal.ca, provides HRM-specific information about nutrition and community resources for people needing nutritional support. Students already receiving dedicated nutritional training include pharmacy (PHAR 2045.015), health and human performance (HPRO 2250.03), and dental hygiene (DEHY 2809.03), and students from medicine and other professions could benefit from the expertise their colleagues are developing. As such, an interprofessional experience centred around a nutrition concern such as obesity might be an ideal meeting ground for the different health professions to discuss and explore practical options for providing collaborative care.
Physician confidence in their abilities depends on their training (Mihalynuk, Scott, and Coombs, 2003), and we at Dalhousie have both the capacity and responsibility to provide skill-building educational experiences to facilitate this confidence. Working together with the Faculties of Dentistry and Health Professions to improve nutrition training of all health sciences students, Dalhousie Medical School has the opportunity to continue and expand our national leadership in education for the health of those we seek to serve.
References
Adams MK, Lindell, KC, Kohlmeier M, and Zeisel SH. 2006. Satus of nutrition education in medical schools. American Journal of Clinical Nutrition. 83(4): 941S-44S.
Appel LJ, Brands MW, Daniels SR, et al. 2006. Dietary approaches to prevent and treat hypertension: a scientific statement from the American Heart Association. Hypertension. 47(2):296-308
Chew F, Grant W, and Tote R. 2004. Doctors on-line: using diffusion of innovations theory to understand internet use. Family Medicine. 36(9):645-50
Conroy MB, Delichatsios HK, Hafler JP, and Rigotti NA. 2004. Impact of a preventive medicine and nutrition curriculum for medical students. Americal Journal of Preventive Medicine. 27(1):77-80.
de Lorgeril M, Salen P, Martin J, Monjuad I, Delaye J, and Mamelle N. 1999. Mediterranean diet, traditional risk factors, and the rate of cardiovascular risk factors after myocardial infarctions: final report of the Lyon Diet Heart study. Circulation. 99:779-85.
Deen D and Margo K. 2007. Nutrition and the Primary Care Clinician. in: The Complete Guide to Nutrition in Primary Care. Malden, Mass: Blackwell Publishing Ltd.
Eaton CB, Goodwin MA, and Stange KC. 2002. Direct observation of nutrition counseling in community family practice. Americal Journal of Preventive Medicine. 23(3):174-9.
Hark LA. 2006. Lessons learned from nutrition curricular enhancements. American Journal of Clinical Nutrition. 83(4): 968S-70S.
Harvey EL, Glenny AM, Kirk SF, Summerbell CD. 2001. Improving health professionals' management and the organisation of care for overweight and obese people. Cochrane Database of Systematic Reviews. (2):CD000984.
Jackson AA. Human nutrition in medical practice: the training of doctors. 2001. Proc Nutr Soc. 60(20):257-63.
Knowler WC, Barrett-Connor E, Fowler SE, et al. 2002. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. New England Journal of Medicine. 346(6):393-403.
Krebs NF and Primak LE. 2006. Comprehensive Integration of nutrition into medical training. American Journal of Clinical Nutrition. 83(4): 945S-50S.
Kushner RF. Barriers to providing nutrition counseling by physicians: a survey of primary care practitioners. 1995. Preventive Medicine. 24(6):546-52.
Martin S. 2004. Younger physicians, specialists use internet more. Canadian Medical Association Journal. 170:1780.
Mihalynuk RL, Scott CS, and Coombs JB. 2003. Self-reported nutrition proficiency is positively correlated with the perceived quality of nutrition training of family physicians in Washington State. American Journal of Clinical Nutrition. 77(5): 1330-6.
National Academy of Sciences. 1985. Nutrition education in US medical schools. Washington, DC: National Academy Press.
Ockene IS, Hebert JR, Ockene JK, Merriam PA, Hurley TG, and Saperia GM. 1996. Effect of Training and a structured office practice on physician-delivered nutrition counseling: WATCH. American Journal of Preventive Medicine. 12(4):252-8.
Ornish D, Scherwitz L, Billings J, et al. 1998. Intensive lifestyle changes for reversal of coronary heart disease. Five-year follow-up of the Lifestyle Heart Trial. Journal of the Americal Medical Association. 280(23):2001–2007.
Touger-Decker R. 2004. Nutrition education of medical and dental students: innovation through curriculum integration. American Journal of Clinical Nutrition. 79: 198-203.
United States Preventive Services Task Force. 2001. Introducing the third US Preventive Task Force. Americal Journal of Preventive Medicine. 20(3S): 3-4.
van Binsbergen JJ, Delaney BC, van Weel C. Nutrition in primary care: scope and relevance of output from the Cochrane Collection. 2003. American Journal of Clinical Nutrition. 77 (4):1083S-1088S.
van Horn L. 2006. The Nutrition Academic Award: brief history, overview, and legacy. American Journal of Clinical Nutrition. 83(4): 936S-40S.
van Weel C. Dietary advice in family medicine. 2003. American Journal of Clinical Nutrition. 77 (4):1008S-1010S.
Weinsier RL, Boker JR, Brooks CM, et al. 1989. Priorities for nutrition content in a medical school curriculum: a national consensus of medical educators. American Journal of Clinical Nutrition. 50:707-12.
Whitlock EP, Orleans CT, Pender N, Allan J. 2002. Evaluating primary care behavioural counseling interventions: and evidence-based approach. Am J Prev Med. 22;267-84.
Woods MN. 2006. Nutrition Academic Award: nutrition education in graduate medical education. American Journal of Clinical Nutrition. 83(4): 971S-75S.