
Heart Murmurs
last authored: Oct 2009, David LaPierre
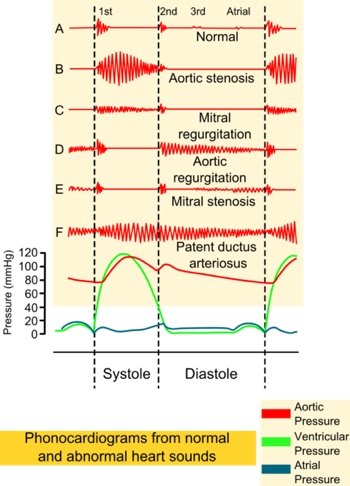
A murmur is an unusual sound generated by turbulent blood flow, resulting from hemodynamic or structural changes to the cardiovascular system. They can become audible or accentuated in high-output states, ie fever or anemia.
courtesy of wikipedia, MadHero88
They are not always a sign of disease, and 50-80% of children will have a murmur at some point.
Murmurs can also suggest structural or functional problems with the heart. Red flags include cardiovascular symptoms, diastolic, pansystolic or continuous murmurs fixed split or single S2, extra sounds, or no change with position.
Murmurs can be caused by various mechanisms:
- flow across a partial obstruction, ie stenosis
- increased flow through normal structures, ie tachycardia
- ejection into a dilated chamber, ie aortic aneurysm
- regurgitation back through an incompetent valve
- abnormal shunting from one chamber to another, ie VSD
Knowing WHERE to listen to heart sounds is very important.
Pitch increases with pressure gradient.
Murmurs can be described by volume, pitch, shape, location, radiation, and response to maneuvers.
- innocent
- systolic murmurs
- diastolic murmurs
- continuous murmurs
- common patterns
Innocent Murmurs
Innocent murmurs have no associated structural problems or ECG/radiological findings.
timing - all innocent are systolic
less than or equal to 3/6
normal physiological split
no extra sounds
radiation to neck or back
they get better with a change in position - "if it goes away, so does the patient"
breath sounds vs murmur?
- ask them to exhale and hold
Innocent murmurs include:
- peripheral pulmonic stenosis (neonatal)
- Still's murmur
- venous hum
- pulmonary ejection
- supraclavicular bruit
Systolic
Systolic murmurs are graded out of 6, while diastolic murmurs are out of 4.
I: very faint
II: soft
III: moderate
IV: loud, with palpable thrill (ie, a tremor or vibration felt on palpation)
V: very loud, with thrill; may be heard when stethoscope is partly off the chest
VI: very loud, with thrill; may be heard with stethoscope entirely off the chest
Ejection Murmurs
diamond shaped - crescendo-decrescendo.
The later the peak in volume, the worse it is.
Innocent murmurs are by far the most common. These often disappear when the person sits upright.
- high frequency, reflexting the sizeable pressure gradient.
- best heard in aortic area at 2nd-3rd right intercostal space.
- typically radiates towards neck, but can often be heard across the chest
- can be harsh
- due to increased flow across pulmonary valve
- best heard at upper-left sternal border
Pansystolic Murmurs
Pansystolic, or holosystolic, murmurs, are caused by regurgitation of blood or through a ventricular septal defect. There is uniform sound intensity throughout systole.
There is no isovolemic contraction, as flow starts immediately.
- continues after A2
- usually flat, but can be crescendo
- best heard at apex, often radiating towarda left axilla
- high pitched and blowing quality
- best heard along left lower sternal border
- the smaller the hole, the louder it is
- best heard at 4th-6th left intercostal spaces
- harsh and high pitched
- may be associated with a palpable thrill
- can stop suddenly; as the muscle thickens
Diastolic
Early diastolic murmurs
Early murmurs result from regurgitant flow through either the aortic or pulomary valve
aordic regurgitation
- high pitched
- begins at A2
- has decrescendo shape, with maximum intensity at onset
- best heard using diaphragm along left sternal border, with person sitting, leaning forward, and exhaling
pulmonary regurgitation
- lower pitched
- intensity may increase with inspiration (why?)
mitral or tricuspid stenosis
- preceded by opening snap
- loudest just after snap
- duration predicts severity
- low pitched; best heard with bell (mtral at apex, tricuspid near xyphoid)
- can have pre-systolic accentuation
hyperdynamic states such as fever, anemia, hyperthyroidism, and exercise can cause increased flow across normal mitral/tricuspid valves and cause a diastolic murmur.
Continuous Murmurs
Continuous murmurs are heard throughout the cardiac cycle and result from conditions where there is a persistent pressure gradient. It is defined as continuing through S2.
venous hums
- generally lower pitched and softer
- combinations of stenosis and regurgitation can lead to a to and fro combined murmur
Patterns to Know
Fixed S2 Split: Atrial Septal Defect
weak/no femorals: coarctation
murmur quieter when sitting (vs lying down): likely normal (innocent)
- usually due toa decrease in venous return
down syndrome: atrioventricular canal defect
Turner syndrome: coarctation of aorta
DiGeorge Syndrome: Tetrology of Fallot
Resources and References
Dal
 |