
Influenza A
last authored:
last reviewed:
Introduction
Influenza has been described as "the last great uncontrolled plague of humankind". Seasonal epidemics continue to cause widespread illness and death worldwide. Massive genetic reassortment periodically occurs and is the catalyst for past and future pandemics. Avian influenza or swine influenza
While many people refer to respiratory infections and even some gastrointestinal infections as 'flu', influenza is caused by the small family of orthomyxoviridae, refering to these viruses' ability to adhere to mucus cells.
The Case of...
Epidemiology
Influenza causes yearly winter epidemics, with birds serving as reservoirs. Health Canada's FluWatch website allows tracking.
between October-March
10%-20% Canadians annually
causes 5,000-10,000 deaths annually
People at increased risk of serious disease include:
- people 65 years of age or older
- residents of a long term care facility
- children 12-23 months
- people under 18 years of age on chronic acetylsalicylic acid therapy
- children and adults with serious chronic conditions (respiratory, cardiac, immunosuppression, renal, malignancy, diabetes, neuromuscular, seizure, cognitive dysfunction, others)
Large pandemics have included:
- Spanish flu (H1N1) 1918
- Asian flu (H2N2) 1957
- Hong Kong Flu (H3N2) 1968
Classification and Characteristics
Influenza A is distinguished based upon its external spike hemagluttinin (HA) and neuraminidase (NA) proteins. Specific viruses are designated HxNx based on the 15 HA and 9 NA protein subtypes. H1N1 and H3N2 are the most common human and swine pathogens.
Influenza viruses are 100-200 nm in diameter and are roughly spherical. Their lipid envelope is covered with about 500 projecting proteins, 80% of which are hemagluttinin and 20% neuraminidase.
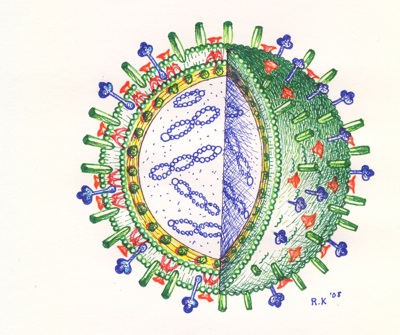 Viral envelope
Viral envelope
Hemagluttinin plays various roles, mediating virus attachment to cell-surface sialic acid receptor and membrane fusion once the virus is inside. It is the primary virl antigen, responsible for the immune response.
Neuraminidase is an enzyme responsible for cleaving sialic acid (mucus) from receptor proteins and liberating the virus from the cell surface.
The virus envelope also contains a small number of membrane protein M2, an ion channel tetramer which modulates virus pH during unpacking.
Viral core
The influenza RNA genome is single stranded, with eight discrete fragments totalling approximately 9 kb in size. These fragments are complexed with proteins including NP, PA, PB1, and PB2 to form helix-shaped ribonucleoproteins (RNPs). These RNPs are surrounded by matrix protein M1, the most abundant structural protien of the virus.
After attachment to cell surface receptors, the virus is endocytosed and transported to endosomes, where the lowered pH leads to HA-mediated fusion of viral and endosomal membranes. The ssRNA is released into the cytoplasm and travels to the nucleus.
Transcription of each of the eight negative-sense RNAs occurs, with six structural proteins and two non-structural proteins formed.
New virions are assembled at the cell surface and are released by budding, with both HA and NA involved. Some cells die, while others undergo many replication cycles.
Transmission and Infection
H1N1 has a incubation period of 1-4 days, average of 2 days, as long as 7 days.
Infection occurs via respiratory droplets and usually begins in the upper respiratory tract. Soiled hands can also transmit the virus with contact of the mouth, nose, or eyes.
The virus adheres to sialic acid glycoproteins or glycolipids in the epithelium of the nose and sinuses, destroying the cilia while multiplying. Secondary spread is possible to muscles, lungs, heart, and elsewhere.
Infection of the lower respiratory tract, leading to pneumonia, occasionally occurs and can be very dangerous. The virus replicates in the alveolar air spaces, leading to exudation.
Key means of avoiding infection include:
- wash hands thoroughly with soap and warm water, or use hand sanitizer
- cough and sneeze in your arm or sleeve
- get your annual influenza shot
- keep doing what you normally do, but stay home if sick
- isolate people suspected of carrying the disease
- avoid crowding (>1m between people)
Clinical Manifesations
After a 2-3 day incubation period, there is an abrupt onset of sore throat, shivering, malaise, headache, and aching in the limbs and back. Fevers tend to be around 39 C. Runny nose and cough tend to be absent. Cytokine release is reponsible for many of the symptoms.
Symptoms typically subside within a week, but in older folks and others at risk, recovery can take much longer, with weakness lasting 3-6 months.
Complications
Primary influenza pneumonia is possible, as is secondary bacterial infection due to tissue destruction, leading to pneumonia or otitis media. Croup or bronchiolitis can also occur in children. Staphylococcus aureus is the most frequent and dangerous agent causing pneumonia, leading to respiratory distress, heart failure, cyanosis, and collapse within days.
Reye' syndrome can follow many viral infections in children, including influenza, and also may involve acetylsalycilic acid (aspirin). It is characterized by encepalopathy and liver failure, and is often fatal.
Complications are more common in:
- elderly
- chronic respiratory diease ie asthma, cystic fibrosis
- chronic heart disease
- immunosupression
- hematological disorders
- chronic renal failure
- chronic metabolic disease, ie diabetes
While most cases of H1N1 resolve after 7-10 days, complications have occasionally been severe. These have included:
- exacerbation of underlying chronic medical conditions
- upper respiratory tract disease (sinusitis, otitis media, croup)
- lower respiratory tract disease (pneumonia, bronchiolitis, status asthmaticus)
- cardiac (myocarditis, pericarditis)
- musculoskeletal (myositis, rhabdomyolysis)
- neurologic (acute and post-infectious encephalopathy, encephalitis, febrile seizures, status epilepticus)
- toxic shock syndrome
- secondary bacterial pneumonia with or without sepsis.
Diagnosis
In general practice, diagnosis is made based upon clinical presentation, along with knowledge of community outbreak.
Samples should be collected with nasopharyngeal swabs or aspirates.
Real-time PCR is the most effective means of identifying flu strain. Other options include antigen testing, immunofluorescence, or viral culture.
Treatment
Amantadine and rimantadine are M2 inhibitors which are useful for seasonal influenza and H1N1.
Oseltamivir (Tamiflu) and zanamivir (Relenza) are neuraminidase inhibitors, acting as sialic acid analogues to inhibit enzymatic activity and slow release of the progeny virions. They are recommended for use against seasonal influenza, as well as H1N1.
The human swine influenza H1N1 appears to be treatable with antivirals:
- oseltamivir (Tamiflu): adults 75 mg twice a day for 5 days; children > 1 year - dosing based on body weight
- zanamivir (Relenza): adults and children >7 years - 10 mg (2 puffs) twice a day for 5 days
It is resistant to amantadine and rimantadine.
Other suggested therapies include ribavarin, interferons, immunoglubulins, and corticosteroids.
Oseltamavir and zanamivir should be started as soon as possible in patients with severe illness.
Vaccines
The yearly trivalent influenza vaccine contains two influenza A strains (H2N3-like and H1N1-like) and one influenza B strain. It is an inactivated (dead) vaccine, produced annually based on antigenic 'trends' that are determined worldwide by the WHO. It takes about 5-6 months to develop a
Its efficacy is:
- 60-80% in young adults
- 20-30% in elderly (lasts 6 months; especially important if seniors travel among regions with different flu seasons.
- 50-60% at preventing hospitalization and pneumonia
Indications
Indications for vaccine include:
- health care workers
- advanced age
- splenectomy
- HIV/AIDS
- lymphoma
- myeloma
- alcoholism
- diabetes
- pregnant women
- infants 6-23 months of age and their caregivers
Two doses one month apart are used in those <9 years of age receiving the vaccine for the first time.
Genetic Variation of Influenza Viruses
Antigenic drift
RNA viruses tend to have mutation rates of more than 10,000 that of DNA viruses, and in the 250 amino acid hemagluttinin protein, two or three substitutions occur each year. These small changes cause seasonal epidemics, especially in the elderly and frail.
H1N1 is triply resorted, with DNA fragments from humans and pigs from both North America and Eurasia. It is a distinct strain, meaning existing vaccines are likely less helpful. It appears to accordingly be the result of significant antigenic drift, not shift.
Antigenic shift
Influenza A viruses readily undergo gene swapping or reassortment due to genome segmentation, and co-infection with two viruses can lead to new virions. The ability of influenza A to infect humans, birds, or pigs, who often live in close proximity to each other, means double infections can lead to unpredictable and dangerous strains. Shift is responsible for influenza pandemics.
Resources and References
- WHO Rapid Advice Guidelines on Pharmacological Management of Influenza Virus. August 2009
- WHO swine flu information
- CDC swine flu information
- PHAC swine flu information
 |