
Heart Sounds
 Heart sounds reveal a great deal about heart function.
Heart sounds reveal a great deal about heart function.
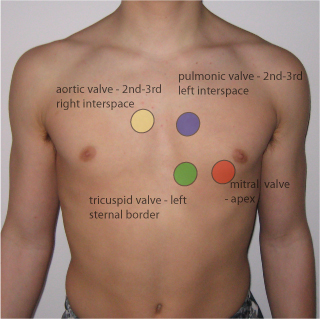
Positions of maximal auscultation
Mitral valve: apex
Triscuspid valve: left lower sternal border
Pulmonic valve: 2nd and third interspaces close to the sternum
Aortic valve: 2nd right intercostal space to the apex
- S1
- S3
- S3
- S4
- abnormal sounds
The First Heart Sound, S1
As the ventricles contract, their pressure rapidly exceeds that of the atria. This forces the tricuspid and mitral valves closed, producing the first heart sound, S1. Because of earlier stimulation of the left ventricle, M1 is slightly before T1, though they are normally indistinguishable. A right bundle branch block may lead to spitting, however.
S1 is heard early in systole. It is high frequency and thus best heard using the diaphragm.
The intensity of S1 is affected by 1) the distance of the valve leaflets, 2) the mobility of the leaflets, and 3) rate of rise in ventricular pressure.
S1 is accentuated by:
- a shortened PR interval: leaflets have not yet begun to drift back
- mild mitral stenosis: prolonged diasolic pressure maintains valves open
- high cardiac output: ie exercise, anemia
S1 is diminished by:
- first degree AV block, with an abnormally long PR interval
- mitral regurgitation
- severe mitral stenosis
- stiffened left ventricle, ie with systemic hypertension
The Second Heart Sound, S2
Further increases in ventricular pressure open the aortic and pulmonary valves, and blood is ejected from the heart. As contraction finishes, pressure falls, and the aortic and pulmonary valves snap shut due to arterial pressure. This produces the second heart sound, S2.
The separation between A2 and P2 vary with the resipratory cycle, a phenomenon called physiologic splitting. One explanation is that during inspiration, the thorax has a greater negative pressure which increases the capacity of pulmonary vessels. This temporary drop in pressure delays the closure of the pulmonary valve, and P2 falls longer after A2. Splitting of S2 is best heard with the diaphragm near the second left intercostal space (pulmonary area).
S2 can be accentuated in people with systemic or pulmonary hypertension, and can be diminished in severe aortic or pulmonary valve stenosis.
Widened splitting, in which there is separation during expiration which grows larger during inspiration, is usually due to delayed closure of the pulmonary valve, as can occur during pulmonary stenosis or right bundle branch block.
Fixed splitting is most commonly caused by an atrial septal defect, in which chronic volume overload of the right heart leads to a high capacitance, low resistance pulmonary system. This delays P2 throughout resipration.
Paridoxical splitting refers to separation during expiration. This is most commonly due to left bundle branch block, whereby there are still normal variations in P2. It can also occur in situations such as aortic stenosis.
Third Heart Sound, S3
S3 is present in early diastole, during the period of rapid ventricular filling. It is a dull, low-pitched sound best heard with the bell. A left-sided S3 is best heard over the apex while the person is lying in the left lateral decubitus position. A right-sided S3 is best heard at the lower-left sternal border, and will change with inspiration.
S3 could be produced by tensing of the cordae tendinae during rapid ventricular expansion. It is normal in children or young adults. In older folks, especially those over 40, it suggests volume overload due to congestive heart failure or increased flow in advanced mitral or tricuspid regurgitation.
Fourth Heart Sound, S4
S4 is present in late diastole and coincides with atrial contraction. It is caused by blood hitting a stiffened ventricular wall.
It usually suggests a loss in ventricular compliance resulting from hypertrophy or myocardial ischemia. It is a dull, low pitched sound best heard with the bell.
Abnormal Sounds
Given their importance, murmurs get their own page!
Ejection clicks
usually close to S1, but do not confuse it with an S1 split
no one really
- caused by restricted aortic or pulmonary valve opening
Aortic clicks are best heard between left sternal border and apex and does not vary on inspiration.
Pulmonary clicks are best heard somewhere else and vary on inspiration.
Opening snaps
Opening snaps are most often caused by mitral stenosis. They are thought to be due to downward bulging and perhaps the abrupt stop of the valves as ventricular pressure drops below that of the atria. It could also be caused by tensing of cordae tendinae when the mitral valve opening.
The interval between S2 and opening snap varies inversely with stenotic severity - the longer the interval, the better their condition.
Quadruple Rhythm
Pericardial Knock
Resources and References
University of Washington bedside teaching