
Acute Abdominal Pain
last authored: August 2009, David LaPierre
Introduction
Up to 20% of people have experienced abdominal pain in the past year. 90% resolve in 2-3 weeks. Only 10% are referred to specialists, and less than 10% are admitted to hospital.
Acute abdominal pain refers to pain with sudden onset and duration of less than 48 hours, while chronic abdominal pain lasts longer than two weeks.
The Case of Mr. Reclu
Mr Reclu is a 54 year-old man presenting to the emergency department with a 2 hour history of intense, constant epigastric pain which began suddenly an hour after lunch. It does not radiate anywhere. He is otherwise healthy, other than intermittent indigestion. He does not take any medications.
What could be causing his pain?
Differential Diagnosis
The most common diagnosis is "nonspecific abdominal pain", usually a self-limited condition with no identifiable cause. However, as many of the potential conditions require urgent surgical involvement, a high index of suspicion is required.
epigastric
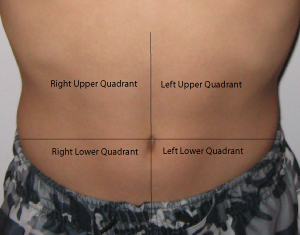
right upper quadrant
right lower quadrant
|
left upper quadrant
left lower quadrant
periumbilical or diffuse
|
History and Physical Exam
- history
- physical exam
History
ChloridePP
Character: colicky pain builds and subsides, suggesting hollow organ pain. Sharp, stabbing pain suggests peritoneal involvement.
Location
epigastric pain can come from the stomach, duodenum, or pancreas.
right upper quadrant pain can come from the biliary tree or liver (cholecystitis)
periumbilical pain can come from the small intestine, appendix, or colon.
sacral pain can come from the rectum.
hypogastric pain can come from the colon, bladder, or uterus.
Onset: Sudden, severe pain suggests perforation (duodenal ulcer) or ischemia, such as can occur with ovarian cyst (perforation or tortion).
Radiation: Pancreatic pain tends to radiate through to the middle of the back. Gallbladder pain tends to radiate around to the right side. Renal pain starts in the flank but can radiate to the groin.
Intensity: rate from 1-10, with 10 being the most severe pain the patient has experienced.
Duration: waves of pain suggest rhythmic muscle contractions, such as those of peristalsis, are involved.
Events Associated: A pertinent review of systems based on the differential.
Provoking and Palliating Factors: The impact of certain behaviours can point to system of origin. Changes with eating, bowel movements, or vomiting suggest pain is GI in origin. Increased pain with exertion suggests cardiac causes.
Associated Symptoms
- fever and chills: inflammation or sepsis
- distension or bloating: intermittent with IBS, progressive with mass or ascites
- weight loss: malignacy or IBD
- change in bowel habits: malignancy
- rectal bleeding
- nausea/vomiting: pain reflex, gastroenteritis, bowel obstruction
- jaundice: liver, biliary tree, gallbladder or hemolysis
- vaginal discharge: PID
past history
- previous episodes
- previous surgery
- medications
- constipation (potentially leading to obstruction)
Physical Exam
The abdominal exam can reveal important clues, and should be started with simple inspection of the state of the patient. An acute abdomen needs to be assessed for immediate surgery.
Weight loss, pignmentation, and signs of dehydration are all possible.
Auscultation can be used to assess bowel sounds and discover bruits.
Palpation should be done gently, starting away from area of pain. Percussion can be used to measure organ size and determine presence of ascites. A pulsatile mass suggests aneurysm, and peripheral pulses should be felt.
Peritonitis is an important finding, first suspected with pain, involuntary guarding or rigidity while taking a deep breath (the most sensitive test). Percussion tenderness may be provocative. Absent bowel sounds are usual, as is rebound tenderness (though this is not sensitive and unnecessarily painful; avoid it).
Right upper quadrant pain can sometimes be associated with a palpable mass in Crohn's disease.
Rectal examination is important to rule out tumour obstruction.
Pelvic examination should be done to rule out pelvic infammatory disease.
Investigations
- lab investigations
- diagnostic imaging
Lab Investigations
CBC: anemia, infection, high platelets in inflammatory disease.
electrolytes, glucose: ketoacidosis, hypercalcemia
liver labs: hepatic or biliary tract involvement
amylase and lipase: pancreatitis
coagulation profile: especially important for people on anticoagulants
b-HCG for pregancy
X-match
tox screen
fecal occult blood test can be used to evaluate potential upper GI bleeds
Diagnostic Imaging
Ultrasound is a fast, safe, and accurate modality to evaluate acute abdomen (Lameris et al, 2009)
Abdominal plain films can detect air under the diaphragm or retroperitoneally from perforation, dilated bowel loops from obstruction, or fecal loading from constipation or obstruction.
ECG should be done to exclude MI.
Endoscopy can be used to detect peptic ulcer disease, gastritis, or tumours, but is contraindicated if perforation is suspected.
barium enemas
HAIDA scans can be used to evaluate gallbladder conditions, but takes time
ultrasound
Management
Supportive care should be provided at once, providing IV fluids as necessary to control heart rate and blood pressure, as well as oxygen if needed.
Pain medications should be provided after an initial examination but before a detailed history and physical exam. Bloodwork should be sent off before clinical evaluation if the situation appears urgent.
Imaging should be postponed until the patient is stable.
Pathophysiology
Abdominal pain results from thermal, mechanical, or chemical stimulation of specific sympathetic nervous system receptors. Visceral neurons are C type, resulting in variable sensation and localization. Peritoneal pain is carred by A and C types, resulting in sharp, localized pain.
Abdominal pain can step from structures in the gastrointestinal, cardiovascular, peritoneal, musculoskeletal, and pelvic systems.
Parietal PainParietal pain originates in the parietal peritoneum and is caused by inflammation. Steady aching pain is more severe than that of visceral pain and can be more precisely localized, as it is carried by somatic nerves. It is typically made worse by movement or coughing, and people tend to want to lie still. Rebound tenderness is present. |
Visceral PainVisceral pain originating in internal organs and structures tends to activate vagus and splanchnic autonomic nerves, with diffuse difficult to localize, typically midline pain. If mucosal, pain tends to be steady - if crampy, visceral pain suggests intraluminal problems.
|
Referred PainReferred pain originates at one location but is felt in another site, superfically or deeply, within or near the same spinal level(s). Abdominal pain can be referred from the thorax, abdomen, pelvis, or spine.
|
The Case of...
Additional Resources
Topic Development
created: David LaPierre, 2008
authors: DLP, Aug 09
editors:
reviewers: