
Renal Function Tests
Renal function tests - most usually serum creatinine (sCr) and blood urea nitrogen (BUN) - are done to estimate glomerular filtration rate (GFR), normally 180L/day.
Cystatin C is a protease which is released into the bloodstream and completely filtered, and may be more reliable but is not as widely used.
Tests that also measure the kidney's ability to maintain salt-water balance can also be used, including fractional excretion of sodium.
- serum
creatinine - blood urea
nitrogen - fractional excretion
of sodium - urine
acidification - protein
excretion
Serum Creatinine (sCR)
Creatinine is a metabolite of creatine, a source of energy in muscle. It is normally produced at a constant rate which varies according to the mass of skeletal muscle. The kidneys filter almost all creatinine, providing a reasonable estimate of GFR.
Normal ranges
- adult males: 53-113 umol/L
- adult females: 37-96 umol/L
- young children: 50 umol/L (increases after age 8 with increasing muscle mass)
- infants: 30 umol/L
- newborns: 37-96 umol/L
There is a non-linear relationship between sCR and GFR, which falls by 50% as sCR doubles. As a 50% decrease in kidney function will send sCR from 50 to 100 umol/L, still within the normal range. Accordingly, it is not sensitive at detecting early kidney disease. Also, normally, only 10% of creatinine is secreted in the tubule. However, as GFR drops, tubular secretion increases up to 40%, increasingly overestimating GFR as renal function declines.
Factors that affect serum creatinine
increases with:
|
decreases with:
|
Calculating Creatinine Clearance
Creatinine clearance will vary among patients (especially for body weight), so it is important to follow creatinine levels over time to correctly determine renal function.
24 Hour Urine Collection
Clearance (mg/dL) is the amount of blood entirely cleared of a solute per unit time = UV/P
- U = urine [Cr]
- V = volume of urine ml/min; divide ml/24h by 1440 to find ml/min
- P = plasma [Cr]
Accuracy is diminished by adequancy of urine collection and the increase in sCr tubular secretion with decreased GFR.
Cockcroft Gault formula
(140-age) x body weight / sCR
x1.2 for males
The CG formula is not as useful for people at extremes of body weight due to difference in muscle mass.
Modification of Diet in Renal Disease (MDRD) formula
GFR = 186/CR-1.154 x age-0.203 units ml/min/1.73 min
x0.742 for females x1.21 for black people
Normal range is 95-105ml/min/1.75m2
Schwarz formula for children
0.55 x height (cm) / sCR
for infants less than 1 year, 0.45 x height (cm) / sCR. Wait until maternal influences have passed.
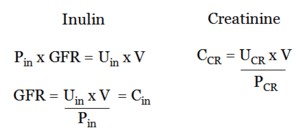
GFR can be measured using a solute such as inulin, a plant sugar, that is freely filtered and neither secreted nor reabsorbed in the tubular system.
Blood Urea Nitrogen
Urea is the major end product of protein metabolism, reflecting protein intake and catabolic rate.
Glomerular filtration excretes urea, but a significant amount is reabsorbed along the tubule and collecting duct, particularly during volume depletion under control of ADH. Accordingly, BUN is more dependent on volume status than sCR.
The normal ratio of BUN:sCr is 10:1. This is increased in a large number of settings:
- volume depletion
- GI hemorrhage
- corticosteroid or cytotoxic agents
- high-protein diet
- obstruction
- sepsis
- catabolic tissue breakdown.
The ratio is increased with liver disease and in people eating a low-protein diet.
normal 2.8-7.8 mmol/L
Fractional Excretion of Sodium
Fractional excretion of sodium (FeNa) is the fraction of filtered sodium that is ultimately excreted and measures tubular handling of a solute relative to GFR.
FeNa = ( UNa / PNa ) ( PCr / UCr )
A value of less than 1% suggests prerenal failure, such as volume depletion, while a value greater than 1% suggests parenchymal renal disease, such as acute tubular necrosis or interstitial nephritis. It may also be less than 1% in people with acute glomerular disease or radiocontrast-induced ARF. Conversely, in patients with persistent vomiting, volume depletion may be seen with high FeNa because of metabolic alkalosis leading to increased urinary sodium. In tihs case, urinary chloride concentration is low and provides an accurate index of volume depletion.
Urine Acidification
Tubular function can be assessed by measuring urine acidification (<5.3) in the presence of systemic acidosis (arterial pH <7.3). Failure to acidify urine suggests distal renal tubular acidosis.
Protein Excretion
Normally, less than 150 mg/day of protein is excreted. Proteinuria can be quantified with either a 24-hour urine collection or with a random urine protein:creatinine ratio. However, because of difficulties collecting urine, a random urine protein / urine creatinine ratio is instead recommended.
Proteinuria is best measured on a 'spot' urine sample, early in the morning.
Urine protein/CR
A random urine protein/creatinine ratio is useful as a screening tool. A ratio of 1 correlates with 1.0 g.
Dipstick
A dipstick is a semiquantitive, low sensitivity measure of protein that detects albumin only. Accordingly, they will miss immunoglobin light chains or Bence Jones proteins seen in multiple myeloma. They are cheap ($0.31 each).
Protein precipitation
Protein precipitation is more sensitive, quantitatively detecting all proteins. It works using sulfosalicylic acid.
Can also differentially asses various protein components.
uromodulin: from luminal surface of TAL
involved in preventing E coli adherence
appears to be involved in some genetic diseases